
“Brain shift makes it impossible to rely solely on the use of neuronavigation.”
We recently shared a blog post featuring Prof. Geirmund Unsgård, Professor Emeritus of Neurosurgery at the Norwegian University of Science and Technology (NTNU). Prof. Unsgård has used ultrasound in neurosurgery for over two decades. Read our previous post here.
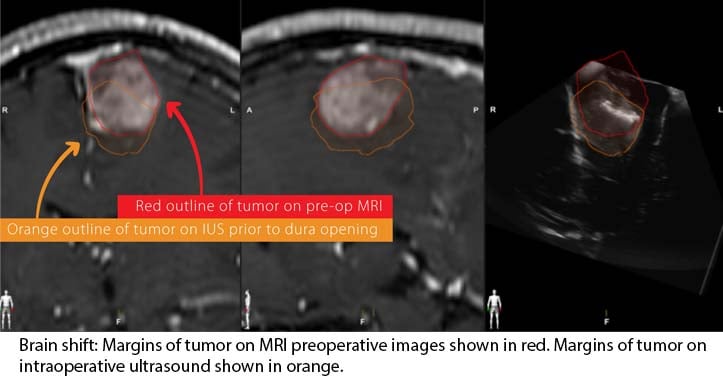
“Brain shift makes it impossible to rely solely on the use of neuronavigation,” says Prof. Unsgård. “It is mostly in tumor resection surgeries where you really cannot use preoperative data. We cannot know for sure how much shift exists. To perform a successful resection, you must be able to see the tumor border and residual tumor at their true locations.” While neuronavigation has become an essential tool in neurosurgery,1 it can lack accuracy and reliability when used intraoperatively.
Because of the brain shift that occurs during procedures, the preoperative data on which neuronavigation systems are based become outdated and unreliable. The change in position of the normal tissue can be considerable and can increase the potential for harm to the patient during surgery.2
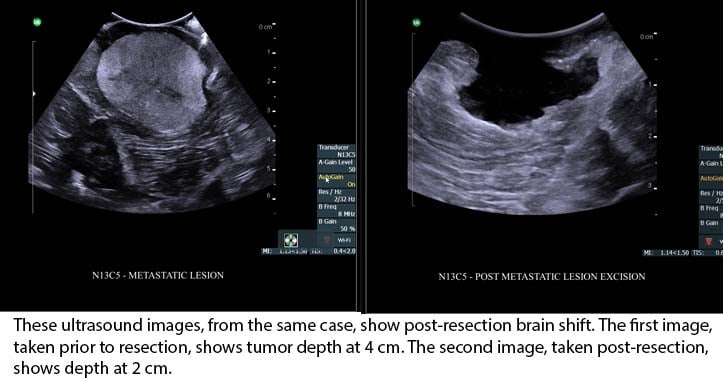
How much displacement can occur? While some studies show mean brain shift in the range of 4 to 8 mm,1 another study reports a maximum brain shift of 10.8 mm prior to opening the dura and a maximum of 15.7 mm after opening the dura.3 According to Prof. Unsgård, it is possible for the brain to shift considerably. “Brain shift due to leakage of cerebrospinal fluid can be near 15 millimeters, and brain shift due to removal of a tumor could be several centimeters, actually.”
Prof. Unsgård encourages the use of intraoperative ultrasound (IUS) to account for brain shift over the course of tumor resection. Current ultrasound technology, such as BK Medical’s bk5000 intraoperative ultrasound system, provides detailed visualization of the true location of the tumor and nearby structures of the brain, helping the surgeon to account for brain shift and update the surgical plan intraoperatively. Unlike intraoperative MR, which can take up to 45 minutes,4 or intraoperative CT, which can take up to 15 minutes,5 ultrasound is the only intraoperative imaging modality that is truly real-time. New ultrasound technology has led to marked improvements in visualization of anatomy. Intraoperative ultrasound designed for surgery, such as that offered by BK Medical, represents a new generation of ultrasound technology, providing clear, highly-detailed images.
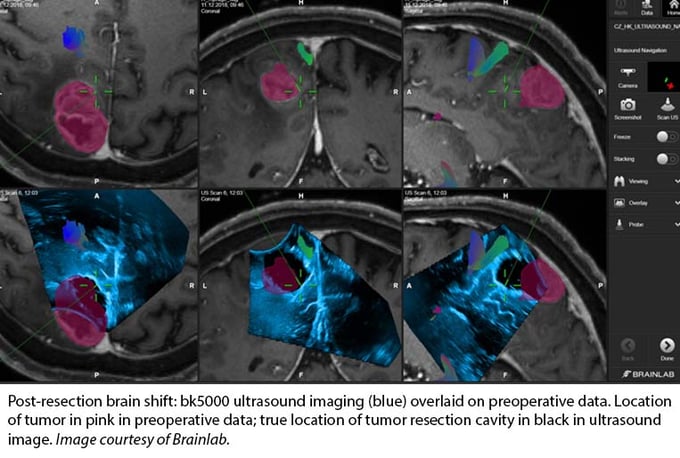
Prof. Unsgård finds ultrasound to be a quick, easy-to-use imaging method that offers excellent image quality. When combined with neuronavigation systems, as with BK’s digital integration with Brainlab Ultrasound Navigation Software, ultrasound can provide updated and accurate images for instant navigation. A real-time overlay of ultrasound imaging on preoperative MR or CT images offers the surgeon accurate, immediate information about brain shift on one screen.
 By visualizing where a tumor really is, surgeons can potentially remove more of the problematic tissue. This is important for patients, says Prof. Unsgård. “It has been more or less proven that the more tumor a surgeon removes, the longer the patient’s lifespan may be. Brain shift makes it really impossible to rely on neuronavigation. In my experience, you can remove the part of the tumor that you see in the ultrasound image with little fear of harming the patient.”
By visualizing where a tumor really is, surgeons can potentially remove more of the problematic tissue. This is important for patients, says Prof. Unsgård. “It has been more or less proven that the more tumor a surgeon removes, the longer the patient’s lifespan may be. Brain shift makes it really impossible to rely on neuronavigation. In my experience, you can remove the part of the tumor that you see in the ultrasound image with little fear of harming the patient.”

[1] Gerard IJ, Kersten-Oertel MA, Petrecca K, Sirhan D, Hall J, Collins L. Brain Shift in Neuronavigation of brain tumours: A review. Medical Image Analysis. 2017;35:403-420. doi:10.1016/j.media.2016.08.007
[2] Bucholz RD, Yeh DD, Trobaugh J, et al. The correction of stereotactic inaccuracy caused by brain shift using an intraoperative ultrasound device. In: Troccaz J, Grimson E, Mösges R, eds. CVRMed-MRCAS’97. Lecture Notes in Computer Science. Springer Berlin Heidelberg; 1997;1205:459-466.
[3] Ohue S, Kumon Y, Nagato S, et al. Evaluation of Intraoperative Brain Shift Using an Ultrasound-Linked Navigation System for Brain Tumor Surgery. Neurologia medico-chirurgica. 2010;50(4):291-300. doi:10.2176/nmc.50.291
[4] https://www.advancedimagingofmt.com/faq/
[5] Zausinger S, Schichor C, Uhl E, Reiser MF, Tonn J-C. Intraoperative CT in Neurosurgery. In: Jolesz FA, ed. Intraoperative Imaging and Image-Guided Therapy. New York, NY: Springer New York; 2014:529-536. doi:10.1007/978-1-4614-7657-3_39